Knowing the Severity of Pectus Excavatum through measuring Haller Index
https://radiopaedia.org/articles/haller-index
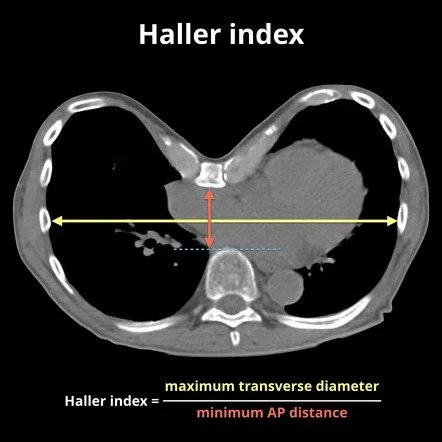
The Haller index (HI), often known as the pectus index, is a simple mathematical method for assessing and describing the chest cage on a CT scan of the thorax. It is used to identify and characterize pectus excavatum.
Measurement and Interpretation of Hallex Index
Imaging is an important component of the evaluation of a patient presenting with pectus excavatum and usually includes non-contrast chest CT (on expiration). CT imaging is important to calculate the Haller index, which is derived by dividing the anterior-posterior diameter by the transverse diameter. This is to determine the degree of chest asymmetry and heart displacement.
The mean calculated index in nonaffected individuals is 2.52; an index greater than 3.25 is considered severe. Additionally, CT imaging provides anatomical information related to chest asymmetry which can be valuable to operative planning.
The Pectus Index is affected by the vertebral level at which it is measured, and it is highest at the cranial level. For consistency, the maximum Haller index in pectus excavatum patients should be calculated by measuring the AP diameter at the deepest point of the sternum.
In the interpretation of the Pectus Index, the following values are used:
normal chest: <2.0
mild excavatum: 2.0-3.2
moderate excavatum: 3.2-3.5
severe excavatum: >3.5
Corrective pectus excavatum surgery is considered with a Haller index ≥3.25
Does High Haller Index require Surgical Repair?
If any two of the following criteria for surgical referral are met, most patients should be evaluated for surgical repair:
Severe deformity as noted by Haller index greater than 3.25
Evidence for cardiopulmonary disability
Decreased peak anaerobic VO2
Restrictive pulmonary disease
Right-sided cardiac compression seen by echocardiogram or thoracic imaging
The shift of the heart into the left thorax
Symptoms of severe defect
In addition, significant psychosocial and body-image perception problems should be taken into account when determining the need for surgery.
The two most common approaches to repair are various modifications of the open approach (Ravitch technique) and the minimally invasive approach (Nuss procedure).
The timing of the operation is also an important consideration as the ideal candidates for repair are typically between 8 and 14 years of age. The flexible chest walls of pre-pubertal patients are better suited to reshaping with the pectus bar.
In short, Surgery is best in younger children with severe symptoms. Adult repair, on the other hand, is more challenging, but it can still be done successfully when entrusted to Dr. LoSasso and the team here at The Centers of Excellence for Pectus. Contact Us Today